Accurately measuring liver size is a fundamental aspect of an abdominal ultrasound examination. While experienced sonographers can often estimate liver size visually (gestalt), standardized objective measurements are crucial for documenting hepatomegaly, monitoring disease progression, or assessing response to therapy.
The most widely accepted and reproducible method for routine clinical practice is measuring the longitudinal length of the right lobe of the liver in the midclavicular line (MCL). This article details this technique and common pitfalls.
1. Patient Preparation and Equipment
- Patient Position: The patient is typically examined in a supine position. To improve visualization, the right arm can be raised above the head, which opens up the intercostal spaces.
- Transducer: A low-frequency curvilinear transducer (typically 2–5 MHz) is preferred to achieve adequate depth penetration through the liver parenchyma.
2. Standard Measurement Technique: The Midclavicular Line
The objective is to obtain a true sagittal (longitudinal) view of the right liver lobe in a plane that parallels the patient’s longitudinal axis.
Step A: Establishing the Measurement Plane
The sonographer places the transducer in the subcostal or intercostal space at the midclavicular line. The probe must be strictly perpendicular to the costal margin. The resulting image should show the full craniocaudal extent of the right liver lobe.
Anatomical Landmarks for a Quality Image:
- The Diaphragm: Must be clearly visualized as a bright, echogenic line forming the superior boundary of the liver (the dome).
- The Inferior Tip: The tapered inferior edge of the liver must be visible.
- No Obliquity: The image should not cut obliquely across the liver (see Section 4, Pitfalls).
Step B: Applying the Calipers
Once the correct sagittal image is frozen, electronic calipers are used to perform the measurement.
- Caliper 1: Placed on the most superior point of the liver dome (the diaphragm).
- Caliper 2: Placed on the most inferior tip of the right lobe.
The measurement is the straight-line distance between these two points.
3. Techniques for Optimizing Visualization
Challenges arise when rib shadows obscure the superior dome or the patient’s habitus makes penetration difficult.
The Role of Respiration
Respiratory maneuvers are essential. Asking the patient to take a deep breath in and hold it will displace the liver inferiorly, pushing it below the ribs. This often brings the entire liver dome into view, ensuring that the superior caliper placement is accurate and not underestimated.
4. Critical Pitfalls and Limitations
The greatest source of error in measuring liver size is incorrect probe positioning. If the transducer is angled obliquely rather than sliced strictly in the sagittal plane, the measurement will be inaccurate.
Oblique Slicing Overestimation
The most common mistake is rotating the probe slightly, which creates a non-sagittal “oblique” cut through the liver. In this scenario, the ultrasound beam might travel diagonally across the organ, artificial extending the measured distance. This results in an erroneous overestimation of liver size, even in a normal-sized liver.
This concept is visualized in the comparative diagram (Image 1).
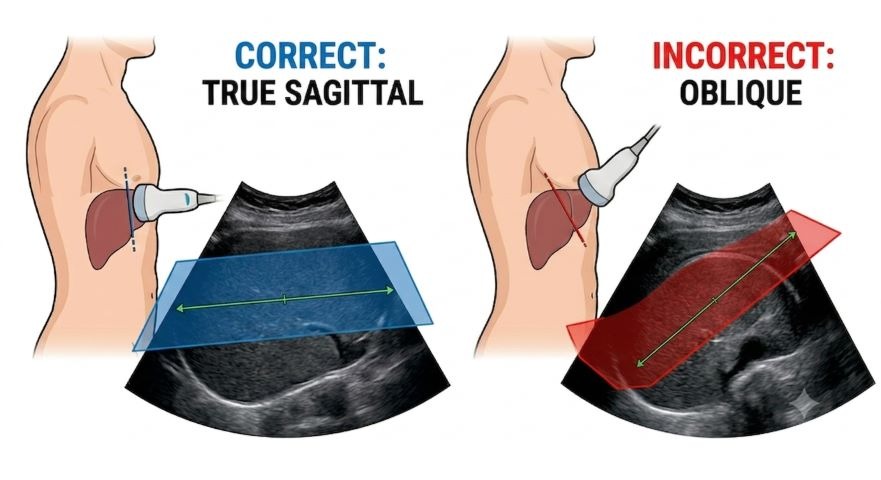
Image 1: Correct vs. Oblique Measurement Planes. Left: The “CORRECT” panel shows the probe perpendicular to the costal margin, yielding the true sagittal MCL measurement (blue slice), identical to the plane used in Image 1. Right: The “INCORRECT” panel shows the probe angled obliquely. This diagonal cut (red slice) creates a falsely elongated section of the liver, leading to an overestimation of its true size.
Other Common Pitfalls
- Failure to Visualize Boundaries: If the liver dome or the inferior tip are not fully seen (e.g., due to bowel gas or poor penetration), the calipers will be misplaced, typically leading to underestimation.
- Assuming MCL is Everything: While the MCL measurement is the standard, it doesn’t capture the shape of the entire liver. A bulky left lobe or a Riedel’s lobe (a normal anatomical variant extending inferiorly) might be missed if the sonographer focuses solely on this single numerical value. Visual assessment and scanning through the entire organ remain essential.
5. Interpreting the Results and Hepatomegaly
What constitutes a “normal” liver size? While ranges exist, interpretation must always be in the clinical context.
- Typical Normal Range: For adults, a measurement up to 15–16 cm in the MCL is generally considered normal. (Values can vary slightly by source, gender, and body habitus; some sources cite up to 13 cm as normal, with 13-15 cm as borderline).
- Hepatomegaly: Measurements exceeding 16 cm in the MCL are indicative of hepatomegaly.
Summary
The standardized ultrasound measurement of liver size at the midclavicular line provides crucial objective data. Success depends on:
- Obtaining a true sagittal image plane (avoiding obliquity).
- Clearly visualizing the diaphragm and the inferior tip (using respiration).
- Accurately placing the calipers at these two defined points.
Mastery of this reproducible technique, combined with a comprehensive visual survey of the entire liver, ensures the most accurate assessment of liver morphology.
Leave a Reply